Yes, Medicare telehealth can cover some dermatology care in 2025, but it depends on the type of visit, the provider, and how the appointment happens. When people say medicare telehealth, they usually mean seeing a clinician by video or sometimes by phone instead of going into an office. For skin issues, that can be great for things like rashes, acne follow-ups, medication refills, and checking a spot that’s changing. But it’s not a perfect fit for every skin problem. In this guide, you’ll learn what Medicare typically covers, where you can be during the visit, what tech you need, and what you might pay.
Best for: Medicare Part B visits where a clinician can evaluate your skin by video and document the visit like an office appointment.
Not ideal when: You need a biopsy, a full-body skin exam, or urgent in-person evaluation for a fast-changing or bleeding lesion.
Good first step if: You’re unsure whether your issue needs an office visit and you want your provider to triage you quickly.
Call a pro if: You get billing you don’t recognize, someone asks for your Medicare number unsolicited, or symptoms suggest an emergency.
Quick Summary
-
Medicare telehealth coverage is mainly handled under Medicare Part B for outpatient-style visits, including many specialist visits.
-
Dermatology telehealth is often used for visual problems, follow-ups, and medication management, but not procedures.
-
You may be able to receive care from home, yet some rules can change based on the service and timing.
-
Video usually works best, but audio-only may be allowed in specific situations with limits.
-
What you pay often looks like a normal Part B visit, unless your Medicare Advantage plan sets different copay rules.
Medicare Telehealth at a Glance
Medicare telehealth is Medicare paying for certain visits delivered remotely. “Telehealth” is the broad term; “telemedicine” often means a video doctor visit, and “virtual visit” means you and the clinician aren’t in the same room.
For Original Medicare, most telehealth coverage runs through Part B (outpatient/medical). Part A is mainly inpatient hospital coverage and is rarely the path for a dermatology telehealth appointment.
Rules for 2025 include temporary extensions of pandemic-era policies, with possible changes later. In practice, confirm visit type, location requirements, and costs before scheduling.
Telehealth vs E-visits vs Virtual Check-ins
Telehealth is the umbrella category. Audio-video visits are live video appointments. E-visits are portal message exchanges over a short time. Virtual check-ins are brief contacts to decide if you need a full visit. They can be billed differently, so your cost may vary.
What Medicare Covers Via Telehealth (Part B)
Medicare Part B generally covers telehealth when it’s a Part B-covered service provided by an eligible telehealth practitioner. In other words, Medicare must already cover the service in person, and the clinician type must be allowed.
For dermatology, telehealth often fits problem-focused care like a new rash review, mole photo evaluation, or medication follow-up. But telehealth doesn’t turn procedures into virtual care. Biopsies, freezing, injections, and full skin exams with dermoscopy usually require in-person visits.
If you’re worried about a spot, comparing melanoma versus a birthmark can help you describe it clearly.
Common Covered Visit Types (Primary Care, Specialists, Mental Health)
Common Part

Where You Can Receive Telehealth (Home, Facilities) and Geographic Rules
Medicare-covered telehealth can often be done from home, but eligibility can depend on the specific service and current rules. Your physical location during the visit may affect whether Medicare pays. Historically, Medicare required certain facilities and limited telehealth to specific geographic areas.
Pandemic flexibilities and later extensions loosened some limits, but some policies have end dates or service-by-service restrictions. If you travel or live in multiple states, ask where you’re allowed to be during the call and whether the clinic needs your address on file.
What “Originating Site” Means (in Plain English)
An originating site is where you are located when you receive telehealth. It might be your home or a facility like a clinic. Medicare sometimes pays only if you’re at an approved originating site, so the provider may need to document your location for billing.
Audio-only, Video Visits, and Technology Requirements
Video visits usually work best for dermatology because the clinician needs to see your skin. An audio-video visit is live sound and video, typically on a phone, tablet, or computer with reliable internet.
You may also be asked to upload photos. Clear images help the provider decide whether telehealth is appropriate or you need an in-person exam. For location-specific concerns, see why acral spots matter before your appointment.
Ask ahead which portal or telehealth platform the clinic uses so you’re not troubleshooting during the visit.
When Phone-only Visits May Be Allowed
Audio-only visits may be allowed in limited situations, such as when you can’t use video, but coverage rules still apply. In dermatology, phone-only fits medication questions or known-condition follow-ups. For a new rash or changing mole, it’s usually inadequate.
Costs and What You’ll Pay
With Original Medicare, telehealth under Part B usually uses the same cost-sharing as an in-person outpatient visit. You generally pay the Part B deductible first. After that, you typically pay coinsurance, often 20% of the Medicare-approved amount.
Costs can still vary by service type, time, and billing codes. The clinic may use telehealth place-of-service codes or modifiers so Medicare knows it was remote.
With Medicare Advantage (Part C), costs may be different because plans set their own copays and rules within Medicare guidelines. Confirm your benefits before assuming you’ll owe “just 20%.”
For skin issues, follow-on costs can include prescriptions or over-the-counter products. If you’re treating eczema, review types of eczema creams so you can ask sharper questions during the visit.
Part B Deductible, 20% Coinsurance, and How Medicare Advantage May Differ
Under Part B, you generally pay the deductible first, then coinsurance (often 20%). Medicare Advantage may use fixed copays and different amounts for primary care versus specialists. Advantage plans may also limit which providers you can use or require referrals.
Special Cases and Key Exceptions to the General Rules
Medicare has exceptions where telehealth may remain available even if other flexibilities tighten. The core idea is that some high-need situations keep broader access.
Telehealth also includes more than live visits. Remote patient monitoring lets clinicians track home-reported health data and is more common in chronic conditions than dermatology.
Because policies can change (including 2026-related dates and extensions into later years), stay flexible. If you rely on telehealth, ask your clinic how scheduling may change and ask your plan what updates could affect coverage.
Behavioral/mental Health, ESRD Home Dialysis, Acute Stroke
Medicare telehealth exceptions often center on access and safety. Behavioral and mental health services are major examples. ESRD home dialysis can also use telehealth for ongoing management. Acute stroke evaluation is another key use case in emergencies when specialists aren’t on-site.
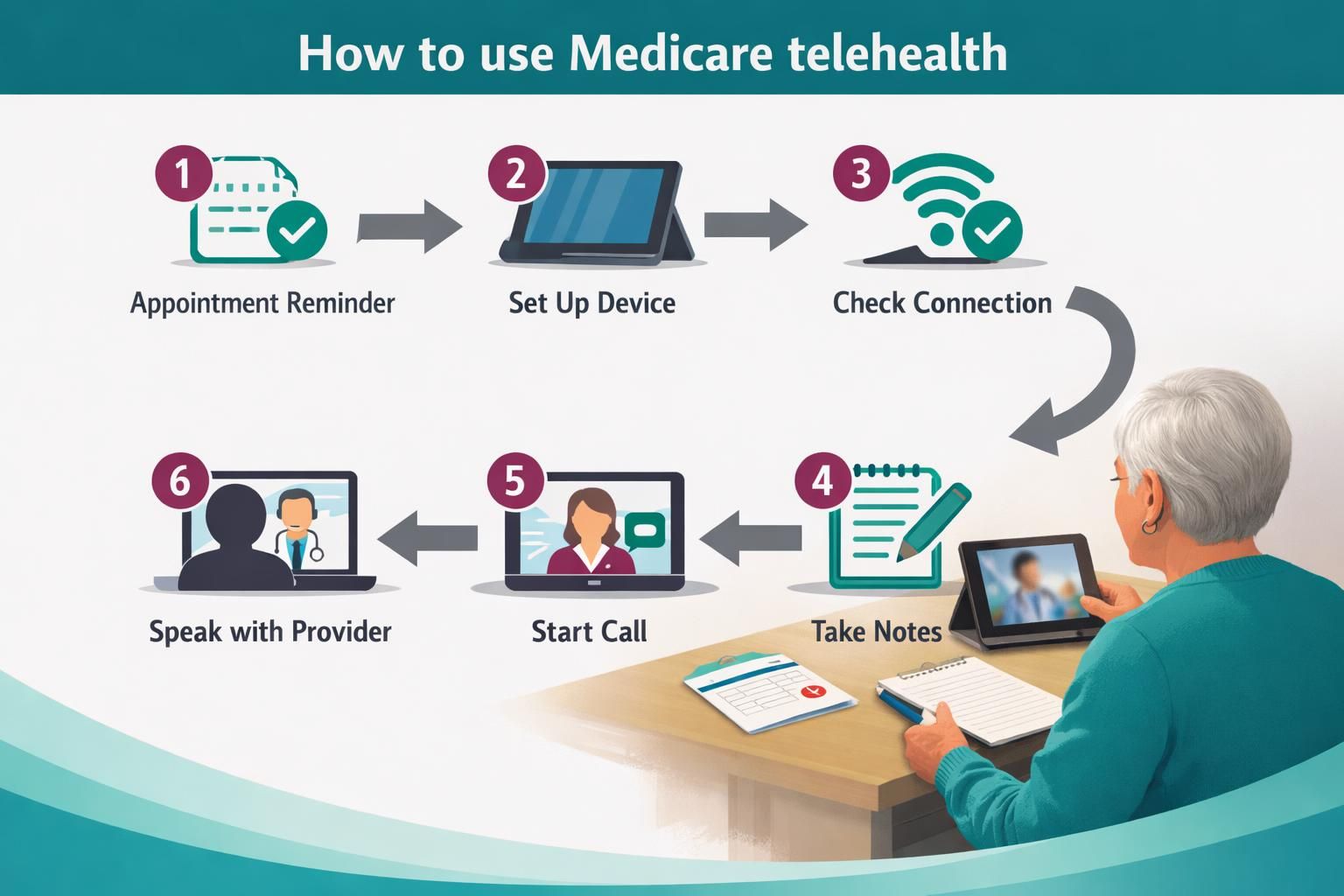
How to Use Medicare Telehealth Safely (and Avoid Fraud)
Use telehealth like any medical visit and protect your personal information. Fraud often involves billing for services you didn’t receive or scam calls pushing you to share your Medicare number.
Schedule only through your provider’s official number or portal. Confirm the visit type and ask whether the clinician accepts assignment. Keep brief notes on the date and what was discussed. Later, review your Medicare Summary Notice or plan EOB for surprises.
If you send skin photos, use the clinic’s secure system, not random texts or unknown emails.
Questions to Ask Your Provider and Red Flags to Watch for
Ask what the visit will be billed as under Part B telehealth, whether photos are needed, and what the next step is if video isn’t enough. Red flags include unsolicited offers, urgency pressure, or requests for your Medicare number. If unsure, contact Medicare or your plan.
Conclusion
Medicare can cover telehealth dermatology in 2025 in many common situations, especially when an eligible clinician can evaluate your concern by video and bill it under Part B rules. Your best next step is to call the office and confirm three things: the visit type, your location requirements, and your expected out-of-pocket cost. Do that, and medicare telehealth becomes a practical option for a lot of everyday skin concerns, while still keeping in-person care available when you truly need hands-on evaluation.